The Corticobulbar Tract
Pass USMLE Step 1, Step 2 CK and Step 3. Only the Best USMLE Prep Program provides the Best USMLE Review Course Content in this rapidly expanding universe of medical information. Become conversant with the new medical discoveries that is transforming our world.
At USMLE Insider Prep Course, we use powerful, illustrative imagery to teach you the challenging concepts that must be mastered for USMLE success. The corticobulbar tract is a poorly understood concept for most medical students. But we make this stuff ridiculously easy. This is what separates USMLE Insider from all the other USMLE Step 1 review courses.
The corticobulbar tract is the major UMN tract controlling brain stem LMNs. It differs from the corticospinal tract as shown in the Table below.
| Feature | Corticobulbar tract | Corticospinal tract |
|---|---|---|
| Cells of origin | Lateral primary motor cortex | Medial primary motor cortex |
| Location in internal capsule | Genu (Fig. 3) | Posterior limb (Fig. 3) |
| Pathway | Crossed and uncrossed (except lower half of face which receives only crossed fibers) | Crossed |
| Target | Brain stem LMN's (V, VII, nucleus ambiguus [of IX, X and XI], XII) | Anterior horn cells of the spinal cord |
The 'bulb' is an archaic term for medulla. That means the cortico-bulbar tract originates from the cortex and ends in the medulla (bulb). The tract has actually been recently renamed corticonuclear tract, to emphasize its projection to brainstem motor cranial nerve nuclei.
The corticobulbar fibers are upper motor neuron (UMN) fibers originating from area 4 of the frontal lobe and running through the genu of the internal capsule to pass through the crus cerebri of the midbrain to end in the medulla. These are fibers of the pyramidaal tract derived from the face areas of the motor cranial nerve nuclei of the pons (trigeminal and facial) and medulla (hypoglossal and the nucleus ambiguus of CN 9, 10 and 11). The corticobulbar projections are as follows:
-
The motor nucleus of CN V receives bilateral input.
-
The nucleus ambiguus receives bilateral projections for the glossopharyngeal (CN IX), vagal (CN X) and accessory nerves (CN XI).
-
The motoneurons of the hypoglossal nucleus which supply the tongue muscles are bilateral (CN XII).
-
However, the facial nucleus of CN VII has two divisions - upper and lower. The upper facial division of CN VII which innervates the upper face receives bilateral projections while the lower facial division which innervate the lower face are mostly crossed. Consequently, a lesion of the corticobulbar tract here results in contralateral lower facial weakness (recall that the upper face receives bilateral input!), tongue (CN XII) and palate (CN X) [see Figure 1].
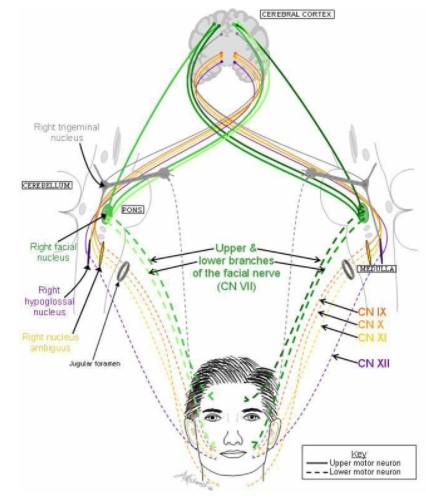
Figure 1. The corticobulbar tract projecting to various cranial nerve motor nuclei. Notice how the facial nucleus of CN VII has two divisions - an upper and lower nuclei - with the upper division (which innervates the upper face) receiving bilateral projection while the lower division (which innervates the lower face) is crossed.

Figure 2. The pink X represents a UMN lesion of the right corticobulbar tract. You should understand how it would cause left lower facial weakness (gray fibers to the left lower face) because the left upper face receives the green input from the ipsilateral side. Understand how the patient's right upper and lower face are not affected by this lesion.
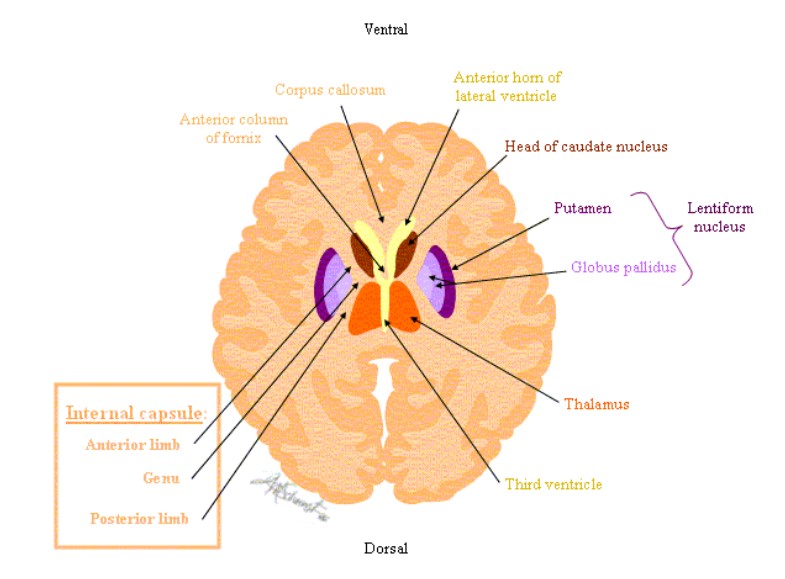
Figure 3. Take note of the genu and posterior limb of the internal capsule in the above Figure. The corticobulbar tract passes through the genu of the internal capsule while the corticospinal tract passes through the posterior limb of the internal capsule.
Facial Paralysis due to Corticobulbar tract (UMN paralysis)
As stated previously, a lesion of the corticobulbar tract results in contralateral lower facial weakness (recall that the upper face receives bilateral input!). This lesion is above the facial nucleus of CN VII and interrupts the corticobulbar fibers to the motor nucleus of the facial nerve. If the facial nucleus or nerve itself (lower motor neuron) were to be lesioned, it would result in paralysis of both ipsilateral upper and lower face (Bell palsy).
Bell Palsy (LMN Facial paralysis)
Interruption of CN VII peripherally at the stylomastoid foramen will interrupt the motor component of CN VII but leave the secretory and sensory components of CN VII intact. Bell palsy is therefore not commonly accompanied by deficits in cutaneous sensation.
The facial nerve (CN VII) innervates the entire side of the face, including the eyebrows and eyelids. If the CN VII is lesioned, the entire face becomes paralyzed. There will be an inability to wrinkle the forehead and close the eye (because of paralysis of the orbicularis oculi). Usually the eyelids are sutured together in an operation called tarsorrhaphy to protect the cornea (because of loss of the blink reflex, which is a protective reflex) until the time that regeneration of the nerve occurs. The patient will not be able to retract the lip and saliva may drool from the corner of the mouth. There may also be hyperacusis (abnormal loudness of sound) if it involves lesion of the branch to the stapedius muscle, which normally dampens sound waves. There may be loss of taste on the anterior two-thirds of the tongue and reduced lacrimal salivary secretions. During regeneration, there may be a misdirected growth of regenerating salivary and lacrimal axons that will cause the so-called 'crocodile tears,' in which the patient tears on eating, instead of salivating.
Now, check out one of the USMLE questions we have prepared on these concepts. At USMLE Insider Prep Course, we have our experts stimulate your mind with challenging questions. Not only are our USMLE course notes one to die for, but we create the fertile atmosphere for your brilliant mind to flourish. We stimulate you to think critically and help you not only achieve the highest score on the USMLE but also to be a great clinician. This is why many consider our program the best USMLE review course out there. Test yourself with this and let us see how you do. We will discuss the answer and offer explanations later.
1. A 57-year-old bank executive suffers a stroke. He has a long-standing history of hypertension but has not been compliant with his treatment regimen. The patient, who is also a smoker, is conscious on examination. The left lower part of his face is paralyzed and he has hemiplegia on the left side, with equal paralysis of the arms and leg but no cognitive deficits are noted. The cranial nerve examination is unremarkable. Where in the nervous system is his lesion?
A. Left brain stem
B. Right brain stem
C. Frontal lobe on the right side
D. Frontal lobe on the left side
E. Left internal capsule
F. Right internal capsule
G. Left thalamus
H. Right thalamus




